I’m reading a lot about hormesis and I think it is an interesting lens to look at improving on multiple medical problems. I’m going to throw out some hypotheses just cause I’m thinking a lot about it. Would love thoughts on applying the hormetic idea to other issues in the comments.
Hormesis is the stimulation of a beneficial, physiologic response after exposure to mild stress from a source normally thought of as harmful. The most well known example would be physical exercise. We go and lift weights and/or run to induce a cellular response to the stress, resulting in a positive impact on the body. What is routinely glossed over is the stress that exercise places on the body. Physical exercise results in a 20x increase in respiration in the body’s mitochondria to produce the energy needed to do work. This has serious negative implications, increasing the production of harmful substances such as reactive oxygen and nitrogen species, other free radicals, acids, and aldehydes.
The body has to fire up the detoxification system to remove these harmful molecules, repair DNA that has been damaged by the reactive species, and adapt to the exercise stress. The time of exercise itself doesn’t produce the majority of positive effects (no, those 250 calories you “burned” aren’t the important part,) it’s the body’s overshooting with the repair mechanisms that results in the net gain. I think so many people think of exercise as a chance to “burn off” calories/donuts/pasta/beer; however, the benefit of exercise comes at the expense of the increase in metabolism. We fire up the mitochondria and “burn off” calories (a harmful stress) to get the repair benefits at the DNA and protein production level. The calorie usage (very small for an hour of exercise in comparison to our resting metabolism) is the price we pay to get all sorts of terrific detoxification enzymes, higher levels of the antioxidant system Glutathione, and DNA repair tools created. This just struck me as a neat way to think about it, exercise as a dose, a means to an end, not an end in itself.
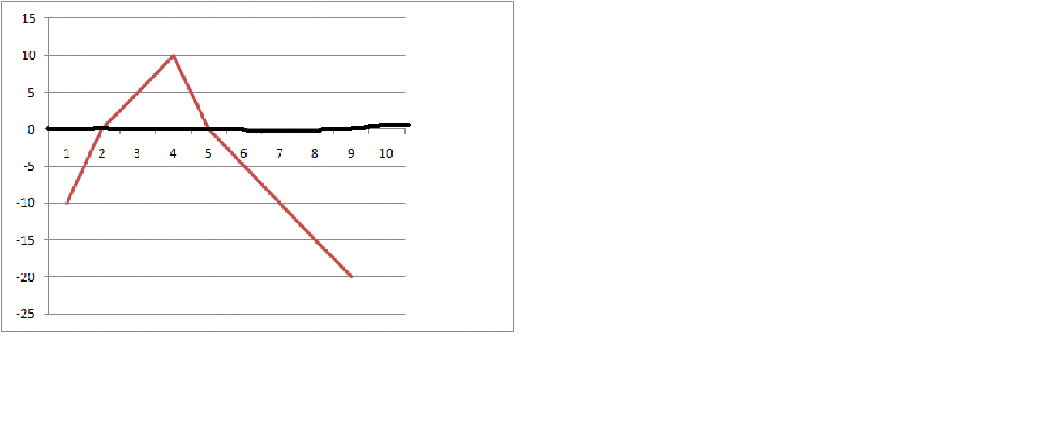
Why is it important to view exercise this way? Because Michelle Obama and others believe exercise is a tool to create a caloric deficit. Is the current trend to fight excess with excess in America and the plan to tackle obesity (in children no less) with increased exercise. I think the hormetic response curve shows why this logic is flawed. Almost every stress that induces a hormetic response, like exercise, follow this pattern.

As you can see, the red line is the physiologic response to increasing amounts of stress (exercise). Above the black, x-axis, there is a benefit to the organism. Below the x-axis there is net harm. Increasing amounts of the stress are not necessarily good. There is a narrow range where the benefits outweigh the harm. In viewing exercise as beneficial because of the caloric deficit created, you ignore the physiologic balance that must be taken into account, and could end up doing more damage than good.
You can apply this same thinking to other stressors. For example, my grandpa and I have talked a lot about sun. He has got me thinking about sun energy as a “dose” that follows a similar hormetic response curve. Sun is great in small doses, even prevents skin cancer to some degree by revving up DNA repair enzymes in the skin. What have we done? Slop molecules that become reactive species on our skin, let them intercalate into the DNA, and stay in the sun for excess dose anyway.
Take alcohol, I do think that it is a poison. However, why has it been repeatedly shown that people that drink 1-2 drinks a day live longer with less disease than abstainers? Hormesis… The moderate dose of alcohol needs to be dealt with, revving up the detoxifying mechanisms in the liver and creating a net positive response. This tips in favor of harm as you lean towards higher dose, leading to the harmful effects of alcohol. Once again we see the hormesis response curve.
What else do you think follows this dose response curve? Short term fasting, cell phone radiation to the head, periodic gorging on food, sugar exposure? All little stressors at an optimal dose. I think it is a neat way of viewing human interaction with the surrounding environment, hormetic response.
The trick is to find that sweet spot, the positive hormetic response brought about where the dose is higher enough but not too high. I think this is where the heart of the n=1, personal hacking, experiential endeavor into finding your best self lies.












{kind=link}